
There is one condition that strikes fear into every dietitians’ heart; one which causes a whole host of cardiac, respiratory, liver, kidney, GI, muscular and metabolic issues, but to name a few. A condition solely caused by nutrition (or lack thereof), which can kill you in a matter of hours. One which we are trained to spot as early as possible, before the symptoms have even started. I’m talking about refeeding syndrome.
What is Refeeding Syndrome?
Refeeding syndrome has been around for millennia, but it only came into the general publics consciousness after World War II. The horrors of concentration camps across Europe were beginning to be uncovered; people who were sick, starving, emaciated. These people, once liberated, were fed to help them gain weight and recover from the atrocities that they endured; but despite surviving months or years in the concentration camps, they started dying soon after being released. Why?
During Starvation
When we enter a period of starvation, our body is running on empty. We begin to slow down biological processes in order to conserve energy and to conserve nutrients needed to create energy, so that we can sustain ourselves for longer.
Within the first 24-48 hours of no nutrition, our glycogen stores (stores of carbohydrate in the muscle and liver) deplete. We end up with no more of this after a very short period, due to the body preferring this type of energy- glucose.
Once these stores have been depleted, our body begins to turn towards ketosis to survive. Essentially, protein and fat stores begin to be depleted to produce ketones, which can be used as an energy source for the brain.
When we use ketones for energy, we require the use of a significant amount of different electrolytes; potassium, magnesium, phosphate, alongside some others. They begin to deplete as starvation takes a hold. Whilst we do have stores of each of these nutrients within our cells to a certain extent, we don’t have infinite supply; so if we aren’t replacing these electrolytes, total body amounts of them deplete. Despite this, our blood levels of all of these will remain fairly steady and stable (unless incredibly severe starvation occurs); this is because our blood requires a very specific amount of each of these nutrients in to maintain homeostasis (balance), and prioritises this as much as possible.
During this time, our BMR (basal metabolic rate) depletes, in a process known as adaptive thermogenesis. Essentially, the body stops all non-essential functions that use energy, and prioritises only the live saving measures.
Breaking the Fast
When we reintroduce food after a period of little to no nutrition, many different processes occur;
- The insulin surge; consuming carbohydrates post-fast causes a rapid increase in blood sugar levels. The body responds to this by secreting insulin, to help bring the levels down.
- Electrolyte imbalance; insulin drives the glucose into the cells, but also drives potassium, phosphate and magnesium into the cells too. For the average person who is consuming these electrolytes regularly, this is no big deal; theres enough in the cells to prevent this happening too fast, but for someone who has been starved or who has fasted, the levels just aren’t there. This leads to low amounts of these nutrients within the bloodstream (known as hypokalaemia, hypophosphataemia and hypomagnesaemia). Equally, higher levels of carbohydrate utilise thiamine (vitamin B1) for carbohydrate metabolism- whilst not an electrolyte, it is still essential for refeeding syndrome.
- Sudden increase in metabolic rate; suddenly, the body doesn’t know what to do with this abundance of energy, and it begins to upregulate its metabolic rate again. This worsens the electrolyte imbalances.
What Does This Do to The Body?
These massive imbalances in electrolytes and thiamine have huge consequences for the body.
Heart issues
All of the electrolytes, especially potassium, are essential for the proper functioning of the heart. Refeeding syndrome can lead to arrhythmias, heart failure, and cardiac arrest (a complete stopping of the heart).
Breathing problems
Electrolyte imbalances can lead to respiratory depression (less breathing), and phosphate in particular can lead to acute ventilatory failure (complete stopping of breathing). The rapid rise in glucose can lead to oedema (fluid) in the lungs, as can a lack of thiamine.
Liver issues and Kidney problems
Low phosphate in particular can cause liver dysfunction. People with refeeding syndrome often urinate a lot more than usual due to the imbalances in blood sugars and electrolytes. They cannot concentrate their urine as effectively. At the same time, their ability to filter things through their kidneys is diminished, and acute kidney injury or tubular necrosis can occur.
Gastro issues
Nausea, vomiting, diarrhoea and constipation are all common symptoms, depending on which electrolyte is increased or decreased. Equally, complete paralysis of the bowel (ileus) can also occur.
Neurological and muscular problems
Wernicke’s encephalopathy is very prevalent in those without sufficient levels of thiamine, which causes severe damage to the brain. Paralysis, seizures, weakness, confusion, ataxia and coma can also occur due to low levels of electrolytes. Rhabdomyolysis (breakdown of muscle cells) can also occur.
Metabolic dysfunction
Less oxygen can get to tissues from the blood. Acid levels rise within the blood leading to metabolic or lactic acidosis (which can kill if not treated). Low levels of other electrolytes such as sodium and calcium can also occur.
Essentially, refeeding syndrome is an emergency. Experiencing refeeding syndrome can very easily kill you if not treated as soon as possible.
How Do We Manage Refeeding Syndrome?
Dietitians in hospital are trained to be able to identify people at risk for refeeding syndrome, and treat them appropriately. Those who are at risk have the following:
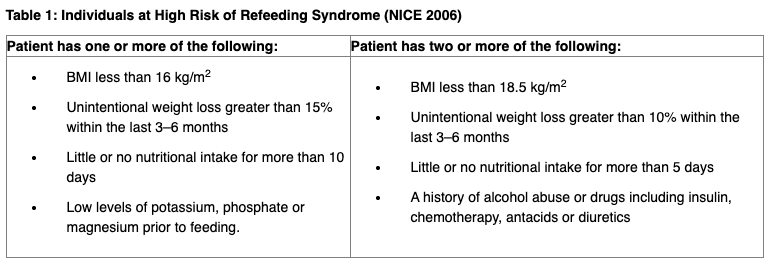
We manage refeeding syndrome based on risk. Essentially, everyone who is deemed at risk of refeeding syndrome is given the following nutritional supplement protocol to reduce the risk of it developing:
- A multivitamin and mineral supplement OD (once per day- such as Sanatogen A-Z or Forceval Soluble)
- 200-300mg thiamine OD (once per day)
- Vitamin B co-strong TDS (three times per day)
At the same time, reinstating of nutrition is done based off of risk factors:
- Moderate risk: 15-20kcals/ kg / day, increasing over 3-5 days until normal intake resumed.
- High risk: 10kcals/ kg/ day, increasing over 3-5 days until normal intake resumed.
- Very high risk: 5kcals/ kg/ day, increasing over 5-7 days until normal intake resumed.
If electrolytes begin to drop, oral supplementation of potassium (Sando K), a magnesium IV or a phosphate tablet (Phosphate-Sandoz).
Overall, refeeding syndrome is a very, very serious condition, which should never be taken lightly. Dietitians are trained to identify it, and prevent it from happening before it starts.
Photo credit: Surajit Sarkar on UnSplash
